J Health Behav Med Hist 2025:1-7 PDF
The evolution of a behavioural model: how the triangle shaped my thinking
Robert C. van de Graaf, MD, director
MEDTCC Institute for Health, Behaviour, Medicine and its History, The Netherlands.
Some ideas arrive suddenly, in a moment of inspiration. Others take years to form, growing through experiences, challenges, and unexpected discoveries. The ‘TOPFIT Behavioural Model’© and ‘TOPFIT Behaviour Triangle’© belong to the second category. It was not a single breakthrough, but rather a long evolution – shaped by key moments in my upbringing, education, medical career, and personal life.
A childhood fascination with behaviour and work
My interest in behavioural dynamics began long before I became a medical doctor. My father was a Human Resources manager, and his work fascinated me. Our home was filled with books on psychology, leadership, and workplace behaviour, and I often found myself flipping through them, curious about what drove people’s actions.
Even as a child, I questioned why some people thrived at work or in school while others struggled. I wondered how much their environment shaped their success and what role context played in developing talent, whether in sports or in a career. Most of all, I was fascinated by the idea of control – how much influence did people really have over their own habits, choices, and life paths?
At the time, I didn’t realize it, but these early questions planted the seeds for what would later become my central focus: understanding the dynamic relationships between people, tasks, and their environment.
The animal within: how nature shapes our behaviour
Years later, as a medical student and skilled field hockey player, I became acutely aware of how much of our behaviour is automatic. The moment I stepped onto the field, a switch flipped – I didn’t think, I just acted. It wasn’t conscious decision-making but deeply ingrained instinct. Most of what we do follows this pattern: we rely on routines, adapt to groups, and avoid discomfort, even when change is necessary. My conclusion was clear – our nature shapes our behaviour.
Eager to understand why, I studied the emerging field of (evolutionary) psychology. It confirmed what I had already sensed: human behaviour is largely driven by subconscious processes. The brain operates on two levels – an instinctive, fast “animal brain” that controls most decisions and a slower, rational “human brain” that can override it, but only with effort. Most people, most of the time, rely on their automatic brain.
I also realized that every behaviour we exhibit at any given moment, in any given context, has more advantages than disadvantages – otherwise, we wouldn’t do it. This is the essence of behavioural psychology. Whether it’s clinging to habits, resisting change, or making seemingly irrational choices, there is always an underlying balance of pros and cons.
These insights transformed my approach to behaviour change. Rather than relying on facts and persuasion – especially when working with patients struggling with lifestyle-related health issues – I shifted my focus to reshaping (social and physical) environments, starting with my own and recognizing myself as part of my patients’ environment, and vice versa [Van de Graaf, 2022]. When the surroundings support the right choices, behaviour often changes naturally.
Discovering the triangle: a framework for complexity
A crucial moment came around 2006 when I was pursuing a career in plastic surgery and working on a PhD about its history. During my research, I came across professor Jacalyn Duffin’s book ‘Lovers and livers, disease concepts in history’ [Duffin, 2005], where she used a triangle to explain the concept of ‘disease.’ That simple yet powerful framework transformed how I saw medicine. It was no longer just about diagnosing and treating conditions – it was about understanding the relationships between individuals, their complaints, and the (medical) environment. Throughout history, diseases have come and gone; they are not fixed entities.
I started seeing this triangular dynamic everywhere. In plastic surgery – especially in cosmetic procedures – it became clear that we weren’t just responding to medical needs; we were also creating demand with our techniques. Some colleagues developed new methods and then shaped the perception that people needed these treatments. Was that really so different from the alcohol or food industries, which influenced consumer behaviour to fuel their own business models? It made me wonder: are we creating diseases as much as we are treating them?
That idea – that medical problems don’t just exist but are shaped by their context, including the medical context – stayed with me. And so did the triangle. It became a tool to clarify complex issues, not just in medicine but also in understanding human behaviour, including my own.
Applying the triangle to an addiction care facility that reeked of smoke
The next major shift came in 2012 when I left the hospital setting and moved into youth addiction care. At DOK3, a secure juvenile care facility in Groningen in the north of the Netherlands, I was shocked by what I saw. Children as young as ten, who had entered as non-smokers, left as heavy smokers. My colleagues – professionals in addiction care – smoked with them. There was even an in-house tobacco shop where residents could buy cigarettes with the pocket money we gave them.
It was a paradox: how could a facility designed to treat addiction openly encourage one?
Determined to break this cycle, I made it my mission to make the facility smoke-free – not just to prevent children from picking up smoking as a result of our own habits, but also to motivate everyone to quit. This decision later laid the foundation for the smoke-free healthcare and the smoke-free generation movements in the Netherlands.
At DOK3, I saw human behaviour in its rawest form. Both the teenagers and my colleagues acted according to the same fundamental tendencies. Most behaviours were automatic, shaped by habit rather than conscious choice. People followed group norms, even when those norms were harmful. And when confronted with change, they resisted, reacting to discomfort as if it were pain.
Changing behaviour meant disrupting not just individual habits but also the routines of the group – the “herd” – that had come to rely on those shared patterns. When I introduced smoke-free policies, the resistance was overwhelming. It wasn’t just the teenagers who pushed back; the staff did too. Their reactions mirrored withdrawal symptoms: irritability, defensiveness, and even aggression. The discomfort of breaking the routine was so intense that it became clear how deeply ingrained behaviour really is.
Most of what we do is not the result of rational decision-making but of automatic processes. People, most of the time, rely on their instinctive brain. Behaviour emerges from routines, group dynamics, and environmental cues.
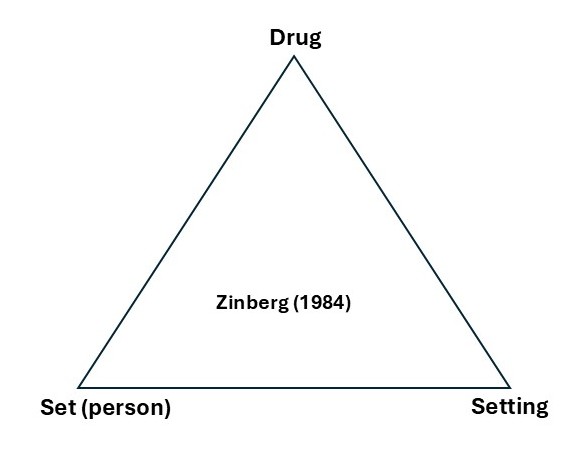
The process of making the clinic smoke-free reinforced what I had already learned: behaviour is shaped by three elements – the person, the substance, and the environment. Another triangle. I came across this same concept in Norman Zinberg’s classic book Drug, Set, and Setting [Zinberg, 1984], which became an essential guide in implementing the smoke-free policy. Zinberg’s book, a classic in addiction care and prevention, echoed the same fundamental truth: the drugs and person cannot be seen separated from its context. All three factors shape user behaviour and experience.
Refining the triangle: the role of relationships
By 2015, I was no longer just applying the triangle – I was refining and expanding it. To inspire my colleagues in healthcare to follow the example of DOK3, the first completely smoke-free healthcare facility in the Netherlands, I organized the Smoke Out Healthcare (Rook de Zorg Uit) conference in October 2015 in Groningen. It was the first smoke-free health care conference in the Netherlands. There, I met Professor Jaap van der Stel, an addiction historian whom I had invited to give a lecture on the history of smoking in addiction care. During his talk, he highlighted a crucial insight: the quality of the relationships between the three elements – substance, person, and environment – determines how likely someone is to seek treatment. Van der Stel made me understand Zinberg’s message even better. His perspective made me reconsider how relationships between key factors shape behaviour.
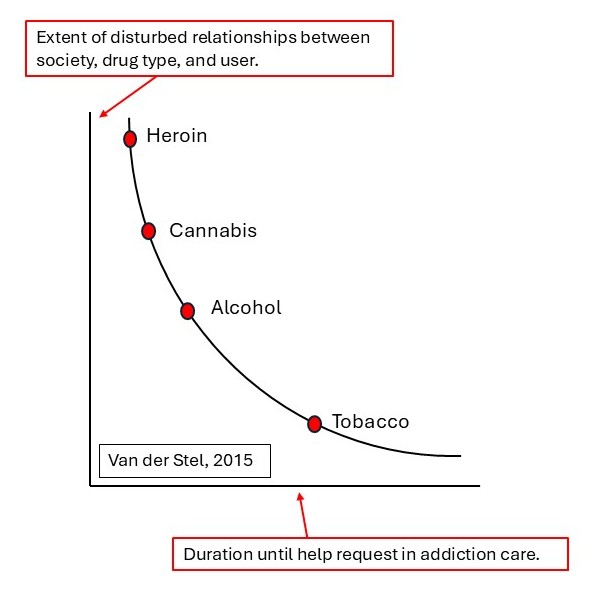
For example, when the connection between alcohol, the person, and their environment is weak -due to strict regulations, social disapproval, or limited availability – fewer people drink, and those who do are more likely to seek help when needed. But when this connection is strong – such as in a culture where drinking is normalized and alcohol is easily accessible – fewer people even recognize excessive drinking as a problem, allowing consumption to continue unchecked.
This same triangular relationship could explain why certain unhealthy behaviours – such as smoking, poor diet, or excessive screen time – persist while others fade away. The weaker the bond between a product and its surrounding, the less likely people are to engage in it.
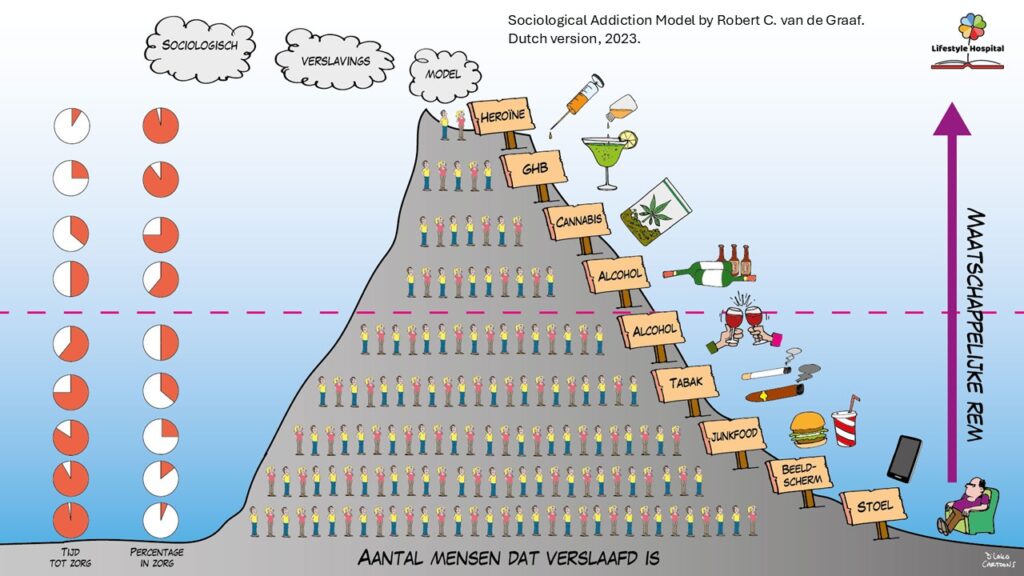
For years, I applied this model in lectures, scientific publications, and behavioural interventions – not only in my clinical practice but also in helping organizations become smoke-free and in my public health work with the Dutch government. It became the foundation of my professional actions and played a key role in the smoke-free healthcare and smoke-free generation movements. I developed a framework around this concept, which I called the Addiction Triangle© or Lifestyle Triangle ©(Van de Graaf, 2016, 2022), as part of my Sociological Addiction Model ©(Figure below) [Van de Graaf, 2016].

Although the Sociological Addiction Model© further developed during the years, something about the model still felt incomplete. Like Zinberg and Van der Stel, I had built it around three key elements – person, environment, and substance (or consumer product). While this interaction influenced behaviour, I wanted a model that included behaviour itself. I wasn’t there yet.
I also wanted to incorporate intrinsic and extrinsic motivation, as well as the role of ability – both internal capacities and competencies and external opportunities. My work as an addiction medicine specialist had shown me how crucial these factors are in shaping behaviour. They needed a clear place in the model. But how?
Rethinking Behavioural Theories
At the start of 2019, I set out to develop a new approach to treating smokers within addiction care. I needed a simple yet effective behavioural model – one that could distinguish between individuals who would benefit from smoking cessation coaching and those requiring specialized addiction treatment. This search led me to the work of Professor Robert West, whom I knew personally from the addiction field. His research on Behavior Change Techniques (BCTs), the Behavior Change Wheel, and the COM-B model [West, 2013; Mitchie 2014] became a key reference point in my exploration.
By chance, while browsing a bookshelf at a consultancy firm, I came across the work of Professor Theo Poiesz [Poiesz, 1999] and discovered the Triad Model [Poiesz, 2014]. This sparked a deeper exploration of various “three-factor” models, further broadening my understanding of behavioural theories.
Each model on behaviour and behavioural change had its strengths, but none felt entirely complete. Many were designed for specific behaviours or contexts, limiting their broader applicability. Some were effective at the public health level but impractical for one-on-one consultations. No matter how promising they seemed, something always felt missing.
Even well-established models like COM-B, Triade, and MOA had a fundamental flaw: they treated behaviour as the outcome of three interacting factors but placed motivation solely within the individual, overlooking external influences. This, I realized, was a critical gap. A more comprehensive approach was needed.
Then came 2020 and COVID-19, and everything changed. My work shifted, my company took a new direction, and my home life and routines were upended. Despite my expertise in behaviour and behavioural change, I struggled to maintain my own performance and well-being. Even my lifestyle habits declined – I couldn’t adapt as well as I had hoped.
More importantly, the models I had relied on offered little guidance in navigating this period. Like much of the world, I was experiencing stress, but I lacked a structured framework to make sense of it. Beyond simply doing my best, taking my time, accepting uncertainty, and breathing deeply, I had no real strategy. As someone immersed in the science of behavioural change, this realization was both frustrating and eye-opening.
One day, after a conversation with my father, I found myself reminiscing about how I used to browse his Human Resources books as a child. That’s when I came across FIT-thinking in current HR literature – and suddenly, everything clicked.
Work behaviour happens within the context of an organization. By reframing behaviours – such as smoking at work – as tasks and viewing the environment as the organization, things became much clearer. The distinction between work and private behaviour wasn’t as rigid as I had assumed. A private environment functions much like an organization – it has people, a culture, a structure, and goals, even if they aren’t always explicitly defined. A family, for example, has an implicit goal: raising children in a healthy way.
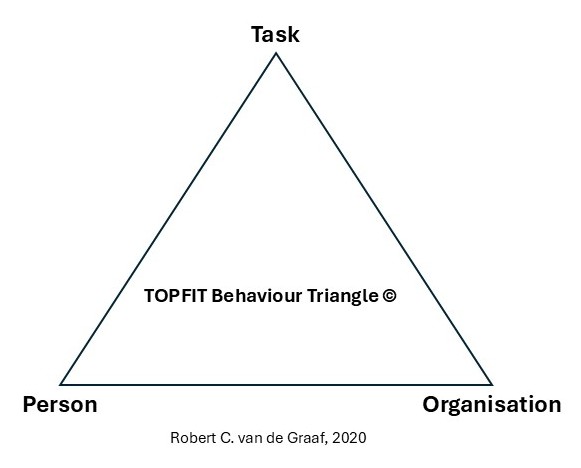
Inspired, I grabbed a marker and drew a simple triangle on the whiteboard in my office. I labeled the three points: behaviour, person, and environment. That was the moment everything started to fall into place. This realization refined my thinking even further. Behaviour – what we do – is not merely a product of several actors and influences but an essential part of the equation itself.
And so, the TOPFIT Behavioral Model© was born, built around three key actors – T (Task), O (Organization), and P (Person)—with their mutual FIT as the crucial factor. In future articles, I will delve deeper into the details of this model.
References:
- Duffin J. Lovers and livers. Disease concepts in history. Toronto: University of Toronto Press 2005.
- Poiesz TBC. Gedragsmanagement. Waarom mensen zich (niet) gedragen. Wormer Inmerc BV 1999.
- Poiesz T. Redesigning psychology. In search of the DNA of behavior. Den Haag: Eleven International Publishing 2014.
- Van de Graaf RC. Smoking, curiosity and value driven personal leadership. Lecture at the Honours Program, University of Groningen, May 10th 2016.
- Van de Graaf RC, Kuitert M. De rol van de zorgprofessional. In: Cahn W. et al. Leefstijl Psychiatrie. Houten: Bohn Stafleu van Loghum 2022:333-61.
- West R, Brown J. Theory of addiction, 2nd edition. UK: Wiley Blackwell 2013.
- Mitchie S, Atkins L, West R. The behaviour change wheel. A guide to designing interventions. Great Britain: Silverback Publishing 2014.
- Zinberg NE. Drug, Set, and Setting. The basis for controlled intoxicant use. New Haven: Yale University Press 1984.
J Health Behav Med Hist 2025:1-7 PDF
Reacties
Eén reactie op “The evolution of a behavioural model: how the triangle shaped my thinking”
[…] de Graaf RC (2025-1). The evolution of a behavioural model: how the triangle shaped my thinking. J Health Behav Med Hist […]