Robert C. van de Graaf, Performance Medicine Specialist, Director MEDTCC Institute for Health, Behaviour, Medicine and its History, and Perform Health Clinic ,The Netherlands
It is almost too strange for words.
For decades we have known that being ill is not the same as being unable to work. That sickness absence is not a disease, but a situation — a pause in the working relationship, not a diagnosis in the body.
And yet we continue to steadily build an entire care system around not working.
A stepped-care treatment model with intake, triage, referral, and aftercare. A parallel healthcare system staffed by sickness-absence physicians, complete with protocols, evaluations, and functional prognoses.
In effect, we have created a new branch of medicine:
the medicine of not working.
It has its own consulting rooms and its own language.
People speak about work capacity, phase-1 and phase-2 reintegration. There are treatment plans, interventions, multidisciplinary meetings.
And above all: there is funding.
Because this illness literally pays.
Those who do not work continue to receive their salary, have a right to privacy, and are protected by a system that is not allowed to ask questions about the cause of the absence from work.
The employer may ask nothing, the employee need say nothing, and the occupational physician mediates between two worlds that no longer look at each other directly.
A Risk Area
Thus one of humanity’s oldest activities — working — has gradually become a risk area, while not working has become a socially recognized condition.
We do not quite call it a disease, but everything about the way we deal with it breathes medicine: diagnosis, treatment, recovery, prevention.
Of course there are people who are genuinely ill, who cannot work because of their illness, where sickness absence and disease coincide temporarily or for longer.
For them, the protection of this system is valuable and justified.
But for a growing group, something else is happening.
The illness is not in the body, but in the way we have organized work.
And that may make not working the ultimate behavioral disease of our time.
A disease that settles not in tissue, but in language, rules, and habits.
A disease perfectly suited to a society that prefers to register rather than reflect, that prefers to treat rather than question.
A Condition
The occupational physician is caught in that logic.
He treats not working as if it were a condition, while often sensing that it is something else:
a person out of balance, an organization that has lost its resilience, a system that has forgotten that work itself can also be part of recovery.
This is where we have gone too far.
We have turned not working into a treatable disease — and that is exactly what we should not want.
Not working is not a disease.
It is a societal symptom, an alarm bell from a system that is running too fast and listening too little.
As long as we continue to medicalize it, we will create more practitioners,
Robert C. van de Graaf, Performance Medicine Specialist, Director MEDTCC Institute for Health, Behaviour, Medicine and its History, and Perform Health Clinic ,The Netherlands
The coalition agreement in The Netherlands is in place. They are getting to work. Building a better Netherlands.
The minimum age for nicotine-containing products will increase. Stocking illegal vapes will become a criminal offense and enforcement will be intensified. Rules around marketing to children will be tightened.
These are not isolated measures. Not a sum of separate policies.
It is one coherent whole.
Not born from moral outrage. Not from a sudden surge of political courage.
But from years of observing one simple truth: behavior can be steered—if you know which levers to turn.
The junk food and nicotine industries no longer need to prove this. They have already run the experiment.
For more than sixty years. On entire populations at once.
Always with the same four controls: the four P’s of the marketing mix— Product, Price, Place, and Promotion.
Turn those controls in one direction, and consumption becomes more attractive, cheaper, more visible, and easier.
What follows is predictable.
Consumption grows.
Reliably. Repeatably. At scale.
No ideology. No debate.
Just technique.
Turn those same controls in the other direction, and the opposite happens.
Consumption becomes less tempting. Less self-evident. A little more difficult.
That too is predictable.
Given that logic, what behavior would you expect to follow?
The World Health Organization has never put it quite this bluntly. It works more cautiously. More slowly as well.
First research. Then evidence. Then consensus. And only after that—after extensive lobbying—policy.
But when you line up WHO recommendations over the years, the so-called Best Buys, something remarkable appears.
Every proven effective measure turns the same controls.
Again and again.
Limit promotion. Change price incentives. Restrict availability. Set standards for the product.
There they are again: the four P’s.
But now in reverse.
That is where behavior emerges.
The coalition agreement makes this concrete.
Take nicotine policy.
Not by appealing to willpower, but by setting limits on the product, restricting access, raising the age threshold, and actively removing illegal variants from the market.
Less availability. More barriers. Less automatic use.
Not paternalism.
Marketing logic— in reverse.
Or look at the tightening of rules around marketing to children.
Not because parents are failing. Not because children simply need to become more resilient.
But because constant exposure normalizes behavior.
Reduce promotion, and the pressure declines.
The environment stops pushing.
That is not a coincidence.
That is exactly how marketing works— this time working against consumption.
The WHO has never framed it this way.
But after years of research the conclusion is clear:
if you want to reduce consumption behavior, you must reverse the marketing mix.
Not halfway. Not temporarily.
But coherently and consistently.
Marketing itself teaches us this:
one lever helps.
Four levers change the system.
This does not require a debate about taste. No moral judgment. No appeal to individual willpower.
It requiresdesign thinking:
which consumption behaviors do we want to reduce— and which do we not?
The industry already gave us the answer. The WHO has confirmed it for years.
Debate 4: Should obesity be considered the disease, or the dysregulated behavioural system?
Robert C. van de Graaf, Performance Medicine Specialist, Director MEDTCC Institute for Health, Behaviour, Medicine and its History, and Perform Health Clinic ,The Netherlands
In contemporary medicine, obesity is widely described as a chronic disease. This framing has played an important role in reducing stigma and legitimising medical care. It has also facilitated the development of pharmacological treatments, bariatric surgery, and specialised obesity care.
However, the behavioural systems perspective raises an additional question: at which level in the causal chain should the concept of disease be applied?
If obesity represents the biological outcome of persistent behavioural dynamics generated within behavioural regulatory systems, it may be argued that the underlying dysregulation occurs primarily within the behavioural system rather than within adipose tissue itself.
From this perspective, obesity may represent one biological manifestation of prolonged behavioural dysregulation.
This observation reveals a potential paradox. Many individuals experience persistent health-compromising behavioural (PHCB) [1] patterns long before obesity develops, yet structured care often becomes widely available only after obesity is present.
A comparable situation exists in addiction medicine, where treatment targets dysregulated behavioural and neurobiological systems rather than waiting for severe somatic complications.
From this perspective, one might ask whether obesity care could also include earlier intervention aimed at behavioural dysregulation itself.
Applying the disease concept to dysregulated behavioural organ functioning could potentially allow earlier intervention, support stepped-care behavioural treatment models, such as in addiction care, and provide a broader framework for addressing health challenges that share similar behavioural dynamics, such as cancer or cardiovascular diseases.
At the same time, important ethical and conceptual questions remain regarding how behavioural dysregulation should be defined and addressed within healthcare systems.
For this reason, the question is not whether obesity should cease to be considered a disease. Rather, the debate concerns whether obesity represents the disease itself – or the biological manifestation of dysregulation within the behavioural system that produces behaviour is the disease.
Debate 3: Do behavioural models compete with medical treatment?
Robert C. van de Graaf, Performance Medicine Specialist, Director MEDTCC Institute for Health, Behaviour, Medicine and its History, and Perform Health Clinic ,The Netherlands
A third question arising from the theory presented in the article Reframing obesity: from adipose tissue disease to behavioural system outcome [1] concerns the relationship between behavioural explanations and biomedical treatments such as pharmacotherapy or bariatric surgery.
Some wondered whether emphasising behavioural regulation might imply that medical treatment is less relevant.
The behavioural organ systems perspective does not oppose medical treatment. On the contrary, it may help explain why certain medical interventions are effective for some patients but not for others.
Pharmacological treatments and surgical interventions modify biological processes that influence behavioural regulation – for example appetite signalling, reward sensitivity, or metabolic functioning. By altering these internal regulatory states, such interventions may help disrupt behavioural feedback loops that sustain persistent health-compromising behaviours (PHCB) [1].
From this viewpoint, biological and behavioural interventions operate at different levels within the same system.
Medical treatments primarily influence biological regulation within the organism. However, biological regulation is only one component of the relational behavioural organ system that generates behaviour through the interaction between organism and environment.
Behavioural therapy therefore represents the broader regulatory approach, within which medical treatments may function as supportive interventions that modify biological conditions influencing behaviour.
These approaches should therefore be understood as complementary rather than competing strategies.
Debate 2: Does focusing on behaviour risk blaming individuals?
Robert C. van de Graaf, Performance Medicine Specialist, Director MEDTCC Institute for Health, Behaviour, Medicine and its History, and Perform Health Clinic ,The Netherlands
Another concern raised in response to the theory presented in Reframing obesity: from adipose tissue disease to behavioural system outcome [1] is that emphasising behaviour might unintentionally reinforce narratives of individual responsibility.
Historically, lifestyle explanations of obesity have sometimes been associated with stigma and moral judgement. The modern framing of obesity as a chronic disease partly emerged to counter such narratives and to acknowledge the complex biological regulation of body weight.
However, within the behavioural organ system perspective behaviour is not interpreted as the product of isolated personal choices.
Behaviour emerges from the continuous interaction between biological processes within the organism and environmental structures that shape behavioural possibilities. Biological predispositions influence how individuals experience hunger, satiety, reward, fatigue, and stress, while environmental conditions influence which behavioural options are available, encouraged, or discouraged.
Modern environments exert particularly strong influences on behavioural dynamics. Highly palatable foods are widely available and heavily marketed, while digital technologies and modern transportation systems substantially reduce the need for physical activity. Social networks and cultural norms further shape patterns of eating, activity, and coping behaviour.
Within the behavioural organ system framework, these environmental structures are not merely external determinants but form part of the behavioural organ system itself. They shape the behavioural landscape within which individuals regulate their actions.
Understanding obesity through behavioural systems thinking therefore highlights the interaction between biological susceptibility and environmental structures, rather than attributing responsibility solely to individuals.
From this perspective, behaviour represents the output of a relational system shaped by biological predispositions, environmental contexts, and learned behavioural patterns.
Debate 1: Does the behavioural systems perspective underestimate biology?
Robert C. van de Graaf, Performance Medicine Specialist, Director MEDTCC Institute for Health, Behaviour, Medicine and its History, and Perform Health Clinic ,The Netherlands
One question raised by readers of the theory of the article Reframing obesity: from adipose tissue disease to behavioural system outcome [1] concerns whether emphasising behavioural dynamics risks underestimating the biological determinants of obesity.
Contemporary research clearly demonstrates that body weight regulation is influenced by complex neuroendocrine mechanisms. Hormones such as leptin, ghrelin, insulin, and cortisol play important roles in regulating hunger, satiety, energy expenditure, and metabolic balance. Genetic variation may also affect appetite regulation, reward sensitivity to food, and metabolic efficiency.
From this perspective, behaviour may appear to be merely the outward manifestation of underlying biological processes.
However, the behavioural systems perspective does not deny these biological mechanisms. Rather, it seeks to clarify how biological signals influence long-term energy balance.
Within this framework, biological processes shape internal regulatory states within the organism. Signals related to hunger, satiety, fatigue, reward sensitivity, and stress influence how individuals experience and regulate eating behaviour, physical activity, sleep, and other health-related behaviours.
Biology therefore remains central to the explanation of obesity. Its influence on body weight, however, is typically expressed through behavioural regulation unfolding over time.
Rather than opposing biological explanations, the behavioural systems perspective aims to connect biological mechanisms with behavioural dynamics within a single integrative framework.
Clarifying the Behavioural Systems Perspective on Obesity. Summary of reader comments and author response
Robert C. van de Graaf, Performance Medicine Specialist, Director MEDTCC Institute for Health, Behaviour, Medicine and its History, and Perform Health Clinic ,The Netherlands
Peter F. van de Graaf, Health Performance Coach MEDTCC Institute for Health, Behaviour, Medicine and its History, and Perform Health Clinic ,The Netherlands
These reactions were not unexpected. The behavioural systems perspective proposed in the article shifts the emphasis within obesity research from adipose tissue as the primary explanatory level toward behavioural dynamics generated within a relational behavioural organ system. Conceptual shifts of this kind naturally invite discussion and critical reflection.
Some readers recognised the value of examining behavioural persistence and feedback mechanisms in obesity. Others raised questions about how this perspective relates to established biomedical models of obesity, the role of biological determinants, and the implications for medical treatment.
Three concerns emerged repeatedly in these discussions. These concerns are addressed below in order to clarify the conceptual intent of the behavioural systems perspective.
Concern 1: Does the behavioural systems perspective underestimate biology?
One concern raised by readers is that emphasising behavioural dynamics might underestimate the role of biological determinants in obesity.
Contemporary research clearly demonstrates that body weight regulation is influenced by complex biological mechanisms, including neuroendocrine signalling, appetite regulation, and genetic susceptibility. Hormones such as leptin, ghrelin, insulin, and cortisol influence hunger, satiety, and metabolic balance, while genetic variation may affect appetite regulation, reward sensitivity to food, and metabolic efficiency.
The behavioural systems perspective does not deny these biological mechanisms. Rather, it seeks to clarify how biological signals influence long-term energy balance.
In this framework, biological processes influence behaviour primarily by shaping internal regulatory states within the organism. Signals related to hunger, satiety, fatigue, reward sensitivity, stress responses, and metabolic status affect how individuals experience and regulate eating, activity, sleep, and other health-related behaviours.
Biological determinants therefore remain central. However, their influence on body weight typically operates through behavioural regulation over time.
Instead of opposing biological explanations, the behavioural systems perspective attempts to connect biological mechanisms with behavioural regulation within a single integrative framework.
Concern 2: Is the concept of a “behavioural organ system” sufficiently clear?
A second concern relates to the conceptual clarity of the term behavioural organ system.
In the article, the behavioural organ is not described as a discrete anatomical structure. Instead, it refers to a relational system responsible for designing and executing behaviour through continuous interaction between the organism and its environment.
Within the organism, biological and psychological processes such as perception, emotion, motivation, reward processing, memory, and stress regulation influence internal states that shape behavioural regulation.
At the same time, environmental structures – including physical surroundings, social norms, cultural practices, and institutional arrangements – shape the behavioural possibilities available to individuals.
In this perspective, the environment is not merely an external determinant of behaviour but a constitutive component of the behavioural organ system itself. Behaviour therefore emerges from the dynamic interaction between organism and environment within this relational system.
The concept of the behavioural organ system is therefore intended as a systems-level framework that connects biological regulation, behavioural processes, and environmental context.
Concern 3: Does focusing on behaviour risk blaming individuals?
A third concern raised by readers is that emphasising behaviour might unintentionally revive narratives that place excessive responsibility on individuals.
Historically, lifestyle explanations of obesity have sometimes been associated with stigma or moral judgement. The modern framing of obesity as a chronic disease partly emerged to counter such narratives and to acknowledge the complex biological regulation of body weight.
However, within the behavioural systems framework behaviour is not interpreted as the product of isolated personal choices.
Behaviour emerges from the interaction between biological processes within the organism and environmental structures that shape behavioural possibilities. Modern environments strongly influence behavioural dynamics. Highly palatable foods are widely available and heavily marketed, while digital technologies and modern transportation systems reduce the need for physical activity. Social networks and cultural norms further influence eating patterns, activity levels, and coping behaviour.
These environmental structures form part of the behavioural organ system itself. They shape the behavioural landscape within which individuals operate.
Behaviour in this framework is therefore understood as the output of a relational system shaped by biological predispositions, environmental structures, and learned behavioural patterns, rather than as the result of isolated individual choices.
Toward an integrated perspective
Taken together, these clarifications highlight that the behavioural systems perspective does not seek to replace biological explanations of obesity.
Instead, it attempts to integrate biological regulation, behavioural dynamics, and environmental influences within a single conceptual framework.
Within this framework, biological processes influence internal states within the organism, environmental structures shape behavioural opportunities, and behavioural patterns determine long-term energy balance.
From this perspective, obesity can be understood as a biological outcome of persistent behavioural dynamics generated within behavioural organ systems operating in modern environments.
Importantly, the relationship between behaviour and obesity is bidirectional. Once obesity develops, physiological and psychosocial changes associated with increased adiposity may further influence behavioural regulation.
In this way, obesity becomes part of the same behavioural feedback system that contributed to its development.
Understanding these dynamics may help bridge the gap between biomedical research on metabolic mechanisms and practical strategies for prevention and long-term health improvement.
Reframing obesity: from adipose tissue disease to behavioural system outcome
Robert C. van de Graaf, Performance Medicine Specialist, Director MEDTCC Institute for Health, Behaviour, Medicine and its History, and Perform Health Clinic ,The Netherlands
Peter F. van de Graaf, Health Performance Coach MEDTCC Institute for Health, Behaviour, Medicine and its History, and Perform Health Clinic ,The Netherlands
Abstract
Obesity is commonly described as a disease of adipose tissue caused by multiple biological, psychological, and environmental determinants, including lifestyle behaviour. While this perspective explains many metabolic mechanisms, it provides limited insight into why the behaviours that drive long-term positive energy balance arise, persist, and prove difficult to change.
In this article we propose a reframing: obesity can be understood as a biological outcome of persistent behavioural patterns rather than primarily as a disease of adipose tissue with many determinants, including behaviour. We introduce a behavioural systems perspective in which behaviour is generated within the behavioural organ system – a relational executive system integrating biological, psychological, social, and environmental influences. Within this system, persistent health-compromising behaviours (PHCB) may emerge and stabilise through reinforcing feedback mechanisms.
A central mechanism underlying these dynamics is the natural comfort loop, in which behaviours that provide short-term relief from discomfort are repeatedly selected. Over time such loops may evolve into the comfort loop syndrome (CLS), where behavioural patterns produce biological, psychological, and social changes that further reinforce the same behaviours.
This framework helps explain the persistence of lifestyle-related health and social problems in modern environments. Viewing obesity through this lens suggests that prevention and treatment should focus not only on adipose tissue or metabolic processes but on disrupting behavioural feedback loops and restoring healthier behavioural regulation within the behavioural organ system.
Introduction
Each year on March 4th, World Obesity Day draws global attention to obesity. Discussions typically focus on body weight, waist circumference, adipose tissue dysfunction, stigma, the many determinants of obesity, and available medical treatments. Yet behind the numbers on the scale lies something more fundamental: patterns of behaviour that gradually develop over time and become embedded in everyday life.
Obesity is commonly described as a disease of adipose tissue. While this biological perspective is important for understanding metabolic mechanisms, it does not fully explain why the behaviours that drive long-term positive energy balance arise, persist, and prove so difficult to change.
In this article we propose a reframing: obesity is not primarily a disease of adipose tissue with many determinants including behaviour. Rather, it can be understood as a biological outcome of persistent behavioural patterns that emerge from interacting determinants and reinforcing behavioural feedback loops.
Viewing obesity through this lens shifts attention from body fat alone to the behavioural systems that shape long-term health. Central to this perspective are two concepts: persistent health-compromising behaviours (PHCB) and the comfort loop syndrome (CLS).
Behaviour as a relational system
Many chronic health and social problems do not arise from a single cause. Instead, they develop gradually from behavioural patterns that emerge within everyday life. These patterns rarely result from isolated conscious decisions. Rather, they arise from continuous interactions between biological processes, psychological states, social influences, and environmental conditions.
In earlier work we described the system responsible for organizing behaviour as the behavioural organ system: a relational executive system that integrates signals from the body, the mind, and the surrounding environment in order to design and execute behaviour [1].
Unlike traditional organs, the behavioural organ is not a single anatomical structure located within the body. Instead, it is a distributed relational system that emerges from the dynamic interaction between the living organism and the world in which behaviour unfolds.
Within the organism it integrates biological and psychological processes such as perception, emotion, motivation, reward processing, habit formation, attention, memory, and stress regulation. At the same time it interacts with the external environment – physical, social, cultural, and institutional contexts – that shape what behaviours are possible, meaningful, or expected.
Behaviour therefore emerges from the continuous interaction between internal states and external conditions. Much of this regulation occurs automatically through learned routines, habits, and behavioural strategies that allow individuals to function in complex and changing environments.
Understanding behaviour as the output of such a relational system helps explain why behavioural patterns can gradually stabilise and persist over time.
Persistent health-compromising behaviours
In this article the term persistent health-compromising behaviours (PHCB) refers to behavioural patterns that negatively affect health and tend to persist because they are reinforced by multiple interacting biopsychosocial feedback mechanisms.
PHCB do not arise from a single determinant. Instead, they emerge from complex interactions between biological, psychological, social, and environmental influences within the behavioural organ system through which behaviour is generated and regulated.
These influences may include genetic predispositions, environmental conditions, psychological distress, physical illness, medication use, social circumstances, and life events such as financial difficulties or relationship breakdown.
Many behaviours that later become problematic initially provide short-term benefits. They may offer comfort, relief from stress, pleasure, or distraction. Eating highly palatable food, for example, may simply be enjoyable, socially rewarding when shared with others, or temporarily reduce emotional tension. Avoiding physical activity may reduce discomfort or fatigue, while sedentary activities such as prolonged screen use may provide relaxation after a demanding day.
From an evolutionary perspective, humans are naturally inclined to select behaviours that reduce discomfort and increase short-term reward. In modern environments characterised by abundant food availability, digital entertainment, and reduced physical demands, these tendencies can easily translate into behavioural patterns that undermine long-term health.
Over time such behaviours may accumulate and lead to negative consequences. These consequences may be physical, psychological, or social. Persistent health-compromising behaviours may contribute to outcomes such as obesity, type 2 diabetes, cardiovascular disease, and certain cancers. They may also contribute to psychosocial consequences including depression, financial problems, relationship difficulties, reduced participation in society, or diminished well-being.
Although these outcomes differ in nature, they share an important characteristic: they often represent downstream consequences of behavioural patterns that gradually emerge from interactions between biological, psychological, social, and environmental processes.
Behavioural feedback loops
A key feature of persistent health-compromising behaviours is that the consequences they produce can themselves become determinants that reinforce the behaviour. In this way behavioural patterns may gradually stabilise or worsen, becoming increasingly difficult to change over time.
For example, financial stress may arise from procrastination behaviours such as avoiding bills while engaging in distracting activities like excessive screen use. The resulting financial pressure can increase psychological distress, which in turn may strengthen maladaptive coping behaviours such as emotional eating, substance use, prolonged sedentary activity, or further excessive screen use.
Similarly, persistent unhealthy eating patterns and sedentary behaviour may contribute to weight gain and metabolic disturbances, including chronic low-grade inflammation, insulin resistance, hormonal alterations in appetite regulation, reduced energy levels, and sleep disturbances. At the same time psychosocial consequences may emerge, including reduced self-confidence, social stigma, and increased stress. These biological and psychosocial changes may further reinforce the behavioural patterns that contributed to them.
A central mechanism underlying many of these processes is the human tendency to seek comfort and immediate relief from discomfort. When individuals repeatedly select behaviours that provide short-term comfort – such as overeating, sedentary behaviour, excessive screen use, smoking, drinking alcohol, or avoidance of effort – these behaviours may gradually form self-reinforcing behavioural patterns.
This process can be understood as the natural comfort loop. Stress, fatigue, boredom, or emotional discomfort trigger behaviours that provide temporary relief or reward. While such responses may be adaptive in certain situations and in the short term, repeated reliance on these comfort behaviours can gradually alter the determinants that influence behaviour.
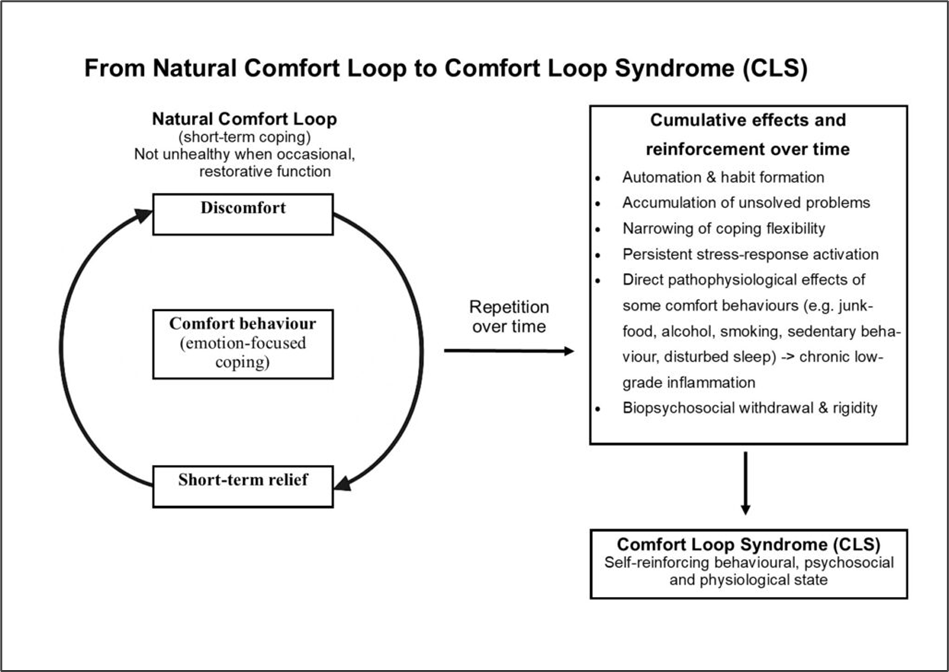
Over time this process may evolve into what we call comfort loop syndrome (CLS). In CLS, behaviours that initially provide relief simultaneously produce biological, psychological, and social changes that increase the likelihood of repeating the same behaviours (Figure 1) [2].
Figure 1. From natural comfort loop to comfort loop syndrome (CLS) [2]
Repeated reliance on comfort behaviours may also lead to automation and habit formation, gradually narrowing the repertoire of available coping strategies. When individuals attempt to change these patterns, biological, psychological, and social withdrawal responses may occur, including increased cravings, irritability, fatigue, and emotional distress.
Through these cumulative effects behavioural loops gradually strengthen, making the patterns increasingly stable and resistant to change.
The obesogenic environment
The current obesity epidemic is strongly influenced by an increasingly obesogenic environment. Highly palatable and energy-dense foods are widely available and heavily marketed, while modern lifestyles provide many opportunities for sedentary behaviour through digital technologies, transportation systems, and changing work patterns.
Human biology and psychology have not fundamentally changed over recent decades. However, the environments in which behaviour occurs have changed dramatically.
From the perspective of the behavioural organ, these environmental changes are highly significant. The behavioural organ is not confined to processes within the individual; it emerges from the continuous interaction between individuals and their environments.
Behaviour is also strongly shaped by social environments. Eating patterns, activity levels, and coping behaviours often cluster within families, peer groups, and communities. Behaviour can therefore spread through social networks, reinforcing shared behavioural norms.
As environments become more obesogenic, the behavioural systems within which individuals operate become increasingly biased toward behaviours that promote energy intake and reduce physical activity. In this way obesogenic environments become embedded within the behavioural organ systems that generate behaviour.
When obesity reinforces behaviour
Once obesity develops, additional feedback mechanisms may reinforce persistent health-compromising behaviours.
Physiological changes associated with increased adipose tissue can influence appetite regulation, metabolism, and energy balance. Hormonal changes may increase hunger signals, while metabolic adaptations may make weight loss more difficult.
At the behavioural level, increased body weight may reduce mobility and increase discomfort during physical activity. Sleep disturbances such as sleep apnoea may contribute to fatigue and reduced energy levels.
Psychosocial consequences may also emerge. Individuals living with obesity frequently experience stigma, social pressure, or reduced self-confidence. These experiences may increase emotional stress and strengthen coping behaviours such as emotional eating or sedentary activities.
Through these mechanisms obesity may become part of the reinforcing feedback system that sustains persistent health-compromising behaviours.
The role of healthcare in reinforcing obesogenic processes
Healthcare systems play an essential role in diagnosing and treating obesity-related diseases. However, certain characteristics of modern healthcare may unintentionally contribute to the persistence of obesogenic processes.
The medical framing of obesity primarily as a biological disease can reduce stigma, but it may also influence motivation by shifting the perceived locus of control away from behaviour. When obesity is presented as the result of many interacting causes – such as genetics, metabolism, environment, and lifestyle – individuals may conclude that they have limited influence over their own body weight. This perception can weaken the sense of personal agency, even though behaviour remains the most direct pathway through which body weight can change.
Healthcare systems also tend to focus strongly on treating the downstream biological consequences of unhealthy behaviour rather than the behavioural processes that generate them. While obesity is indeed influenced by many biological, psychological, and environmental factors, it ultimately develops through behavioural pathways, particularly eating and physical activity patterns. The same determinants that are often described as directly influencing body fat primarily shape behaviour, which in turn determines long-term energy balance and body fat.
Modern medicine has become highly effective at managing many consequences of unhealthy behaviour through medication, surgery, and long-term or lifelong treatment. Although this represents a major achievement of healthcare, it may unintentionally reduce motivation for behavioural change when individuals perceive that health consequences resulting from their own behaviour can be medically managed.
In addition, certain medical treatments themselves may contribute to obesogenic processes. Various medications used for chronic conditions can increase appetite or reduce energy levels, thereby influencing behavioural patterns related to eating and physical activity, resulting in increased body weight.
Taken together, these dynamics illustrate how healthcare systems may unintentionally become part of broader behavioural feedback systems that sustain obesogenic processes.
Discussion and conclusion
The perspective presented in this article reframes obesity as the biological outcome of persistent behavioural dynamics rather than primarily as a disease of adipose tissue. From this viewpoint, body fat accumulation is not the starting point of the problem but the visible biological consequence of behavioural patterns that emerge within the behavioural organ system.
Central to this framework are persistent health-compromising behaviours (PHCB). These behaviours arise through complex interactions between biological, psychological, social, and environmental influences. Because many of these behaviours initially provide short-term comfort or relief, they can gradually stabilise through reinforcing feedback mechanisms. Over time these feedback processes may evolve into what we describe as comfort loop syndrome (CLS), in which behaviours that initially reduce discomfort simultaneously generate biological, psychological, and social changes that increase the likelihood of repeating the same behaviours.
Understanding obesity through this behavioural organ systems perspective has several implications. First, it helps explain why behavioural patterns that contribute to obesity are often highly resistant to change. Behaviour is not simply the result of isolated individual choices, but the output of a relational behavioural organ system that integrates internal states and environmental influences. Once behavioural feedback loops have stabilised, change requires disruption of the reinforcing mechanisms that sustain them.
Second, this framework highlights the central role of the modern environment in shaping behavioural dynamics. Contemporary environments provide unprecedented access to highly rewarding foods, digital stimulation, and sedentary lifestyles. At the same time, behavioural norms spread through social networks, further reinforcing shared behavioural patterns. These environmental conditions increasingly bias behavioural organ systems toward persistent health-compromising behaviours.
Third, the framework illustrates how biological consequences of behaviour, including obesity itself, may become part of reinforcing feedback systems. Physiological adaptations, psychosocial consequences, and environmental responses can all strengthen the behavioural loops that contributed to the condition in the first place.
Importantly, this perspective does not deny the biological mechanisms involved in obesity. Rather, it integrates biological, behavioural, and environmental processes within a single conceptual framework. In this framework, biological processes both influence behaviour and are influenced by behaviour through dynamic feedback loops.
Taken together, this perspective suggests that effective prevention and treatment should focus not only on body weight or adipose tissue, but on the behavioural organ systems that generate persistent health-compromising behaviours. Interventions that disrupt comfort loop dynamics and strengthen healthier behavioural regulation may therefore play a central role in addressing obesity and other lifestyle-related health and social problems.
Ultimately, obesity may be better understood not simply as a disease of adipose tissue, but as a biological footprint of persistent behavioural dynamics unfolding within the behavioural organ systems of individuals living in modern environments.
References
Van de Graaf RC, Van de Graaf PF. The Behavioural Organ. A relational executive system for the design and execution of human behaviour. J Health Behav Med Hist 2026-5.
Van de Graaf RC. Comfort Loop Syndrome: a new framework for understanding and addressing the pandemic of lifestyle-related health societal problems. J Health Behav Med Hist 2025-22.
The Behavioural Organ. A relational executive system for the design and execution of human behaviour
Robert C. van de Graaf, Performance Medicine Specialist, Director MEDTCC Institute for Health, Behaviour, Medicine and its History, and Perform Health Clinic ,The Netherlands
Peter F. van de Graaf, Health Performance Coach MEDTCC Institute for Health, Behaviour, Medicine and its History, and Perform Health Clinic ,The Netherlands
Abstract
Current behavioural models describe interacting determinants of behaviour, yet rarely specify a functionally defined system that produces behaviour as its output. As a result, key phenomena such as effort, stress, persistence, and non-execution remain theoretically under-specified and are often attributed to individual deficits in motivation, self-regulation or capacity.
In this paper, behaviour is conceptualised as the output of a functional executive system: the behavioural organ. This organ is defined as a relational system consisting of the person, the environment, and designed behaviour (task). Its internal anatomy can be visualised by the behavioural triangle. Behaviour is continuously designed within this system and becomes observable only when executed outside it. Whether behaviour is executed effortlessly, with sustained effort, or not at all depends on the quality of relational fit within the system.
By explicitly distinguishing between designed and executed behaviour, and by conceptualising motivation and ability as emergent relational properties rather than individual determinants, this framework offers a novel ontological and functional–physiological account of behaviour. The behavioural organ provides a coherent foundation for understanding effort, stress, and behavioural breakdown as systemic signals rather than personal failures.
Introduction
Behavioural science has produced a wide range of models aimed at explaining why people behave as they do. Determinant-based frameworks such as the Theory of Planned Behaviour, the MOA model, the Triad model [1-2], and the COM-B model [3-4] have played a crucial role in structuring behavioural research, informing intervention design, and advancing prediction and categorisation. Their contribution to the field is substantial and undisputed.
Despite their usefulness, a fundamental question remains largely unanswered: how does behaviour actually come into existence as an executable output?
In most prevailing approaches, behaviour is conceptualised as the result of internal states – such as intentions, motivation, or capacity – moderated by contextual conditions. Behaviour itself is typically treated as a dependent variable: the observable endpoint of interacting determinants. As a consequence, experiential phenomena such as effortful behaviour, stress, persistence, and non-execution are commonly interpreted as failures of motivation, self-regulation, or individual ability.
Importantly, many contemporary behavioural models can be described as system-oriented in a descriptive sense. They acknowledge interaction between multiple determinants and recognise that behaviour does not arise from a single cause. However, they do not propose an ontological system that exists as a functional entity producing behaviour. Behaviour remains conceptualised as an outcome influenced by factors, rather than as the output of a system with an internal architecture, regulatory logic, and execution constraints.
This distinction is not merely semantic. Without an explicit behavioural production system, it becomes difficult – if not impossible – to explain why identical individuals may experience the same behaviour as effortless in one context and exhausting or unsustainable in another, even when motivation appears unchanged. Effort and stress are observed, measured, and intervened upon, but they are not structurally explained.
This paper proposes a different starting point. Behaviour is not approached as a choice, intention, or outcome, but as the output of a functional executive system: the behavioural organ. The term executive is used here to denote behavioural production and regulation at the system level, rather than executive cognitive functions located within the individual.
The behavioural organ framework conceptualises behaviour as something that is first designed within a relational system and only becomes observable when executed outside that system. Whether execution occurs effortlessly, with sustained effort, or not at all depends on the quality of relational fit within the system. In this view, motivation and ability are no longer treated as causal inputs preceding behaviour, but as emergent signals reflecting system coherence.
The present paper is intended as a conceptual and ontological contribution. It introduces the behavioural organ as a functionally specified system with a defined internal architecture and regulatory principles. Empirical operationalisation and validation are explicitly left to future work. The framework builds on a series of earlier conceptual papers that progressively formalised its relational architecture and execution logic.
The need for an ontological shift
The behavioural organ framework introduces an explicit ontological shift. Behaviour is not treated as a property of the person, nor as a direct response to environmental cues, but as the output of a relational system. This shift implies that behaviour must be analysed at the level of system architecture rather than individual determinants.
Within this framework, motivation and ability are no longer understood as causal inputs preceding behaviour, but as emergent properties of relational fit within the system. Effort and stress are not interpreted as failures of self-regulation, but as functional signals indicating misalignment between system components.
The term physiological is used here in a functional–regulatory sense. It refers to energetic cost, compensatory regulation, and system coherence, rather than to specific biological substrates or biomarkers.
To articulate this shift, behaviour is conceptualised through the lens of functional anatomy and physiology. Just as other distributed organ systems are defined by their function rather than by anatomical localisation, the behavioural organ is defined by its role in designing and regulating behaviour.
Intellectual and experiential origins of the model
The behavioural organ did not emerge as a purely theoretical construct. Its development reflects a sustained interaction between clinical practice, behavioural science, organisational contexts, and personal experience.
The relational foundation of the model was first articulated by Van de Graaf in 2025 in his paper entitled Reframing Human Behaviour Through the Behavioural Triangle [5]. Behaviour was conceptualised as emerging from interaction between Person, Task, and Organisation. That paper introduced the distinction between general (abstract) behaviour and visible (executed) behaviour, and emphasised relational quality – friction versus flow – as central to behavioural sustainability.
This framework was subsequently formalised at the level of system ontology in The behavioural organ: an introduction to the system that produces human behaviour [6]. There, the behavioural organ was defined as a distributed functional system spanning organism and world, and the distinction between designed behaviour and expressed behaviour was introduced alongside the energetic logic of fit and misfit.
The developmental trajectory of this thinking was described in The evolution of a behavioural model: how the triangle shaped my thinking [7], situating the model within a longer arc of medical, organisational, and behavioural practice.
Crucially, the present framework was further refined through ongoing dialogue and collaboration with Peter F. van de Graaf, health performance coach and co-author of this paper. These exchanges sharpened the focus on behavioural execution, effort, and sustainability across clinical, organisational, and everyday performance contexts, ultimately leading to the formulation of the behavioural organ as an explicit executive system of behaviour.
The internal architecture of the behavioural organ
The behavioural organ is conceptualised as a functional, non-anatomical organ composed of three elements arranged in a stable triangular architecture: the person, the environment, and designed behaviour (task). This internal architecture can be visualised as the behavioural triangle, which serves as a schematic representation of the anatomy of the behavioural organ (Figure 1).
The person contributes functional capacities and constraints, including skills, energy, needs, and life history. The environment provides structure, culture, norms, goals, and opportunities that shape behavioural demands. Designed behaviour represents the behavioural configuration that emerges from ongoing interaction between person and environment. Crucially, the task is not an externally imposed instruction but an implicit behavioural design reflecting what behaviour is expected and feasible within a given relational context.
Designed behaviour and executed behaviour
A central contribution of the behavioural organ framework is the explicit distinction between designed behaviour and executed behaviour. Designed behaviour refers to the behavioural configuration implicitly prepared within the behavioural organ as a result of person–environment interaction. Executed behaviour refers to the observable enactment of this design in the external world.
This distinction explains why individuals may experience strong intentions, commitment, or responsibility while simultaneously struggling to act – or do not act at all. Behavioural difficulty is not necessarily the result of insufficient motivation but may reflect a mismatch between system components that prevents designed behaviour from being executed without excessive effort.
Fit as the regulatory principle
Whether designed behaviour can be executed depends on the quality of relational fit within the behavioural organ. Fit refers to the alignment between the person and the task, the task and the environment, and the person and the environment. Fit is not an attribute of any single component but a relational property of the system as a whole.
Figure 2 illustrates behavioural execution as a function of relational fit. When fit is high, designed behaviour is executed as designed, effortlessly and sustainably. When fit is partial, behaviour can still be executed but requires sustained effort and increased energetic cost, often experienced as stress. When fit is insufficient, execution fails, resulting in avoidance, withdrawal, or behavioural breakdown.
Behavioural execution is therefore determined by systemic alignment rather than by individual motivation or ability alone.
Repositioning motivation and stress
Within the behavioural organ framework, motivation is not conceptualised as a driver of behaviour but as an emergent signal reflecting system coherence. Motivation tends to increase when relational fit improves and declines when misalignment persists. Similarly, stress is not interpreted as a personal weakness but as a physiological indicator of compensatory regulation under conditions of misfit.
This reframing resolves longstanding ambiguities in behavioural science regarding effortful behaviour, persistence, and apparent resistance to change. Behaviour that is difficult or unsustainable is no longer attributed to individual failure but understood as a predictable outcome of system dynamics.
Implications for behavioural science
By introducing the behavioural organ, this framework provides an explicit ontological foundation for behaviour. It offers a functional explanation for effort, stress, and non-execution and presents a relational alternative to individualised deficit models. Rather than replacing existing determinant frameworks, the behavioural organ complements them by supplying the architectural layer they lack.
Conclusion
This paper introduces the behavioural organ as a functional executive system that designs and regulates human behaviour. By distinguishing between designed and executed behaviour and by locating behavioural success or failure in relational fit rather than individual motivation, the framework offers a novel foundation for behavioural theory. The behavioural triangle makes the internal anatomy of this system explicit, while relational fit explains its functional physiology. Future work will focus on empirical operationalisation, longitudinal dynamics, and applications in health, work, and organisational contexts.
References
Poiesz TBC. Gedragsmanagement. Waarom mensen zich (niet) gedragen. Wormer Inmerc BV 1999.
Poiesz T. Redesigning psychology. In search of the DNA of behavior. Den Haag: Eleven International Publishing 2014.
West R, Brown J. Theory of addiction, 2nd edition. UK: Wiley Blackwell 2013.
Mitchie S, Atkins L, West R. The behaviour change wheel. A guide to designing interventions. Great Britain: Silverback Publishing 2014.
Van de Graaf RC. Reframing human behaviour through the behavioural triangle: a relational systems model for understanding and change. J Health Behav Med Hist 2025-12.
Van de Graaf RC. The behavioural organ: an introduction to the system that produces human behaviour. J Health Behav Med Hist 2025-24.
Van de Graaf RC. The evolution of a behavioural model: how the triangle shaped my thinking. J Health Behav Med Hist 2025-1.
Without a behavioural expert, a weight-loss drug will not work
Robert C. van de Graaf, MD, director MEDTCC Institute for Health, Behaviour, Medicine and its History, The Netherlands
Anne Roefs, PhD. Professor of Psychology and Neuroscience of Abnormal Eating. Faculty of Psychology & Neuroscience, Maastricht University, The Netherlands
In the debate on weight-loss medication, a development has been normalised that is deeply troubling: an organ that is central to obesity is being treated on a large scale by physicians who are not trained to do so. The fact that millions of people may need to use this medication for life makes this painfully clear. Not as a medical success, but as evidence that a complex and vulnerable organ is structurally being treated under the wrong leadership.
The substantial relapse after discontinuation of medication and the prospect of lifelong use are not accidental side effects. They reveal what happens when an organ is manipulated without being truly understood or restored. This is not a failure of patients, nor proof that the medication does not work, but a systemic failure in how we approach obesity.
Obesity does not primarily arise in adipose tissue, the pancreas, or the gastrointestinal tract. It develops in what we might call the behavioural organ: the integrated system in which motivation, reward, stress regulation, impulse control, habit formation, and environmental influences jointly steer behaviour. This organ determines not only what someone eats, but also how they respond to stress, temptation, social pressure, and recovery after relapse. It is learnable and adaptive, but also vulnerable to dysregulation. It is precisely this organ that is now being influenced on a large scale by medication. That is not inherently wrong. It becomes problematic when this intervention is detached from behavioural-medical governance. An organ that organises behaviour cannot be sustainably restored without diagnosis, guidance, and long-term retraining.
In medicine, a fundamental principle applies: the lead clinician is specialised in the organ being treated. A cardiologist does not perform brain surgery; that responsibility lies with a neurosurgeon. An occupational physician does not remove a bowel tumour; that is done by a specialised surgeon. This principle is not a formality, but a basic condition for quality of care and patient safety.
In obesity care, this principle is being abandoned.
Internists, surgeons, cosmetic physicians, and increasingly newly qualified doctors prescribe medication that profoundly interferes with the behavioural organ. This increasingly happens outside regular healthcare, via commercial platforms offering ‘medical weight loss’ as a service. Physicians often act with sincere intentions and follow guidelines or continuing education. But behavioural-medical expertise cannot be replaced by a course, a protocol, or a guideline primarily developed from the perspective of other organs, such as adipose tissue.
Behavioural medicine is a specialty. It requires knowledge of behavioural diagnostics, learning processes, stress and reward systems, contextual influences, relapse mechanisms, and long-term behaviour change. Without this expertise, the complications of the behavioural organ largely remain invisible: loss of self-regulation, dependency thinking, avoidance behaviour, declining resilience, a shift of responsibility from person to product, and dysregulation of stress and reward responses. These are not abstract concepts, but real, long-term consequences that undermine functioning, work, relationships, and health.
The well-known yo-yo effect after stopping weight-loss medication is the most visible signal of this. Weight returns not because individuals fail, but because the behavioural organ has not been restored. That millions of people may require lifelong medication is therefore not proof of effectiveness, but proof that the behavioural organ has structurally remained out of view.
The conclusion is therefore unavoidable: physicians without behavioural-medical specialisation cannot be the lead clinicians in problems of a dysregulated behavioural organ. As with any complex condition, clinical governance belongs with the specialist. Other physicians can support or contribute, but not lead.
If the idea of lifelong weight-loss medication teaches us anything, it is this: obesity does not require ever more powerful drugs, but better governance. Governance that does justice to both the vulnerability and the capacity for recovery of the behavioural organ. And that begins with recognising it as a fully recognized centre of treatment.