J Health Behav Med Hist 2026-6
Reframing obesity: from adipose tissue disease to behavioural system outcome
Robert C. van de Graaf, Performance Medicine Specialist, Director
MEDTCC Institute for Health, Behaviour, Medicine and its History, and Perform Health Clinic ,The Netherlands
Peter F. van de Graaf, Health Performance Coach
MEDTCC Institute for Health, Behaviour, Medicine and its History, and Perform Health Clinic ,The Netherlands
Abstract
Obesity is commonly described as a disease of adipose tissue caused by multiple biological, psychological, and environmental determinants, including lifestyle behaviour. While this perspective explains many metabolic mechanisms, it provides limited insight into why the behaviours that drive long-term positive energy balance arise, persist, and prove difficult to change.
In this article we propose a reframing: obesity can be understood as a biological outcome of persistent behavioural patterns rather than primarily as a disease of adipose tissue with many determinants, including behaviour. We introduce a behavioural systems perspective in which behaviour is generated within the behavioural organ system – a relational executive system integrating biological, psychological, social, and environmental influences. Within this system, persistent health-compromising behaviours (PHCB) may emerge and stabilise through reinforcing feedback mechanisms.
A central mechanism underlying these dynamics is the natural comfort loop, in which behaviours that provide short-term relief from discomfort are repeatedly selected. Over time such loops may evolve into the comfort loop syndrome (CLS), where behavioural patterns produce biological, psychological, and social changes that further reinforce the same behaviours.
This framework helps explain the persistence of lifestyle-related health and social problems in modern environments. Viewing obesity through this lens suggests that prevention and treatment should focus not only on adipose tissue or metabolic processes but on disrupting behavioural feedback loops and restoring healthier behavioural regulation within the behavioural organ system.
Introduction
Each year on March 4th, World Obesity Day draws global attention to obesity. Discussions typically focus on body weight, waist circumference, adipose tissue dysfunction, stigma, the many determinants of obesity, and available medical treatments. Yet behind the numbers on the scale lies something more fundamental: patterns of behaviour that gradually develop over time and become embedded in everyday life.
Obesity is commonly described as a disease of adipose tissue. While this biological perspective is important for understanding metabolic mechanisms, it does not fully explain why the behaviours that drive long-term positive energy balance arise, persist, and prove so difficult to change.
In this article we propose a reframing: obesity is not primarily a disease of adipose tissue with many determinants including behaviour. Rather, it can be understood as a biological outcome of persistent behavioural patterns that emerge from interacting determinants and reinforcing behavioural feedback loops.
Viewing obesity through this lens shifts attention from body fat alone to the behavioural systems that shape long-term health. Central to this perspective are two concepts: persistent health-compromising behaviours (PHCB) and the comfort loop syndrome (CLS).
Behaviour as a relational system
Many chronic health and social problems do not arise from a single cause. Instead, they develop gradually from behavioural patterns that emerge within everyday life. These patterns rarely result from isolated conscious decisions. Rather, they arise from continuous interactions between biological processes, psychological states, social influences, and environmental conditions.
In earlier work we described the system responsible for organizing behaviour as the behavioural organ system: a relational executive system that integrates signals from the body, the mind, and the surrounding environment in order to design and execute behaviour [1].
Unlike traditional organs, the behavioural organ is not a single anatomical structure located within the body. Instead, it is a distributed relational system that emerges from the dynamic interaction between the living organism and the world in which behaviour unfolds.
Within the organism it integrates biological and psychological processes such as perception, emotion, motivation, reward processing, habit formation, attention, memory, and stress regulation. At the same time it interacts with the external environment – physical, social, cultural, and institutional contexts – that shape what behaviours are possible, meaningful, or expected.
Behaviour therefore emerges from the continuous interaction between internal states and external conditions. Much of this regulation occurs automatically through learned routines, habits, and behavioural strategies that allow individuals to function in complex and changing environments.
Understanding behaviour as the output of such a relational system helps explain why behavioural patterns can gradually stabilise and persist over time.
Persistent health-compromising behaviours
In this article the term persistent health-compromising behaviours (PHCB) refers to behavioural patterns that negatively affect health and tend to persist because they are reinforced by multiple interacting biopsychosocial feedback mechanisms.
PHCB do not arise from a single determinant. Instead, they emerge from complex interactions between biological, psychological, social, and environmental influences within the behavioural organ system through which behaviour is generated and regulated.
These influences may include genetic predispositions, environmental conditions, psychological distress, physical illness, medication use, social circumstances, and life events such as financial difficulties or relationship breakdown.
Many behaviours that later become problematic initially provide short-term benefits. They may offer comfort, relief from stress, pleasure, or distraction. Eating highly palatable food, for example, may simply be enjoyable, socially rewarding when shared with others, or temporarily reduce emotional tension. Avoiding physical activity may reduce discomfort or fatigue, while sedentary activities such as prolonged screen use may provide relaxation after a demanding day.
From an evolutionary perspective, humans are naturally inclined to select behaviours that reduce discomfort and increase short-term reward. In modern environments characterised by abundant food availability, digital entertainment, and reduced physical demands, these tendencies can easily translate into behavioural patterns that undermine long-term health.
Over time such behaviours may accumulate and lead to negative consequences. These consequences may be physical, psychological, or social. Persistent health-compromising behaviours may contribute to outcomes such as obesity, type 2 diabetes, cardiovascular disease, and certain cancers. They may also contribute to psychosocial consequences including depression, financial problems, relationship difficulties, reduced participation in society, or diminished well-being.
Although these outcomes differ in nature, they share an important characteristic: they often represent downstream consequences of behavioural patterns that gradually emerge from interactions between biological, psychological, social, and environmental processes.
Behavioural feedback loops
A key feature of persistent health-compromising behaviours is that the consequences they produce can themselves become determinants that reinforce the behaviour. In this way behavioural patterns may gradually stabilise or worsen, becoming increasingly difficult to change over time.
For example, financial stress may arise from procrastination behaviours such as avoiding bills while engaging in distracting activities like excessive screen use. The resulting financial pressure can increase psychological distress, which in turn may strengthen maladaptive coping behaviours such as emotional eating, substance use, prolonged sedentary activity, or further excessive screen use.
Similarly, persistent unhealthy eating patterns and sedentary behaviour may contribute to weight gain and metabolic disturbances, including chronic low-grade inflammation, insulin resistance, hormonal alterations in appetite regulation, reduced energy levels, and sleep disturbances. At the same time psychosocial consequences may emerge, including reduced self-confidence, social stigma, and increased stress. These biological and psychosocial changes may further reinforce the behavioural patterns that contributed to them.
A central mechanism underlying many of these processes is the human tendency to seek comfort and immediate relief from discomfort. When individuals repeatedly select behaviours that provide short-term comfort – such as overeating, sedentary behaviour, excessive screen use, smoking, drinking alcohol, or avoidance of effort – these behaviours may gradually form self-reinforcing behavioural patterns.
This process can be understood as the natural comfort loop. Stress, fatigue, boredom, or emotional discomfort trigger behaviours that provide temporary relief or reward. While such responses may be adaptive in certain situations and in the short term, repeated reliance on these comfort behaviours can gradually alter the determinants that influence behaviour.
Over time this process may evolve into what we call comfort loop syndrome (CLS). In CLS, behaviours that initially provide relief simultaneously produce biological, psychological, and social changes that increase the likelihood of repeating the same behaviours (Figure 1) [2].
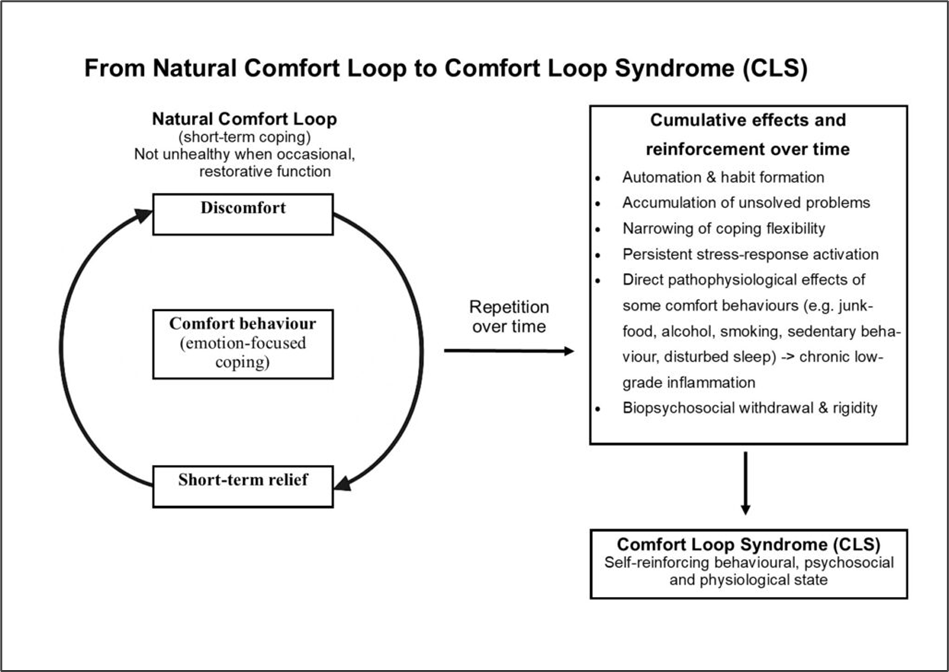
Figure 1. From natural comfort loop to comfort loop syndrome (CLS) [2]
Repeated reliance on comfort behaviours may also lead to automation and habit formation, gradually narrowing the repertoire of available coping strategies. When individuals attempt to change these patterns, biological, psychological, and social withdrawal responses may occur, including increased cravings, irritability, fatigue, and emotional distress.
Through these cumulative effects behavioural loops gradually strengthen, making the patterns increasingly stable and resistant to change.
The obesogenic environment
The current obesity epidemic is strongly influenced by an increasingly obesogenic environment. Highly palatable and energy-dense foods are widely available and heavily marketed, while modern lifestyles provide many opportunities for sedentary behaviour through digital technologies, transportation systems, and changing work patterns.
Human biology and psychology have not fundamentally changed over recent decades. However, the environments in which behaviour occurs have changed dramatically.
From the perspective of the behavioural organ, these environmental changes are highly significant. The behavioural organ is not confined to processes within the individual; it emerges from the continuous interaction between individuals and their environments.
Behaviour is also strongly shaped by social environments. Eating patterns, activity levels, and coping behaviours often cluster within families, peer groups, and communities. Behaviour can therefore spread through social networks, reinforcing shared behavioural norms.
As environments become more obesogenic, the behavioural systems within which individuals operate become increasingly biased toward behaviours that promote energy intake and reduce physical activity. In this way obesogenic environments become embedded within the behavioural organ systems that generate behaviour.
When obesity reinforces behaviour
Once obesity develops, additional feedback mechanisms may reinforce persistent health-compromising behaviours.
Physiological changes associated with increased adipose tissue can influence appetite regulation, metabolism, and energy balance. Hormonal changes may increase hunger signals, while metabolic adaptations may make weight loss more difficult.
At the behavioural level, increased body weight may reduce mobility and increase discomfort during physical activity. Sleep disturbances such as sleep apnoea may contribute to fatigue and reduced energy levels.
Psychosocial consequences may also emerge. Individuals living with obesity frequently experience stigma, social pressure, or reduced self-confidence. These experiences may increase emotional stress and strengthen coping behaviours such as emotional eating or sedentary activities.
Through these mechanisms obesity may become part of the reinforcing feedback system that sustains persistent health-compromising behaviours.
The role of healthcare in reinforcing obesogenic processes
Healthcare systems play an essential role in diagnosing and treating obesity-related diseases. However, certain characteristics of modern healthcare may unintentionally contribute to the persistence of obesogenic processes.
The medical framing of obesity primarily as a biological disease can reduce stigma, but it may also influence motivation by shifting the perceived locus of control away from behaviour. When obesity is presented as the result of many interacting causes – such as genetics, metabolism, environment, and lifestyle – individuals may conclude that they have limited influence over their own body weight. This perception can weaken the sense of personal agency, even though behaviour remains the most direct pathway through which body weight can change.
Healthcare systems also tend to focus strongly on treating the downstream biological consequences of unhealthy behaviour rather than the behavioural processes that generate them. While obesity is indeed influenced by many biological, psychological, and environmental factors, it ultimately develops through behavioural pathways, particularly eating and physical activity patterns. The same determinants that are often described as directly influencing body fat primarily shape behaviour, which in turn determines long-term energy balance and body fat.
Modern medicine has become highly effective at managing many consequences of unhealthy behaviour through medication, surgery, and long-term or lifelong treatment. Although this represents a major achievement of healthcare, it may unintentionally reduce motivation for behavioural change when individuals perceive that health consequences resulting from their own behaviour can be medically managed.
In addition, certain medical treatments themselves may contribute to obesogenic processes. Various medications used for chronic conditions can increase appetite or reduce energy levels, thereby influencing behavioural patterns related to eating and physical activity, resulting in increased body weight.
Taken together, these dynamics illustrate how healthcare systems may unintentionally become part of broader behavioural feedback systems that sustain obesogenic processes.
Discussion and conclusion
The perspective presented in this article reframes obesity as the biological outcome of persistent behavioural dynamics rather than primarily as a disease of adipose tissue. From this viewpoint, body fat accumulation is not the starting point of the problem but the visible biological consequence of behavioural patterns that emerge within the behavioural organ system.
Central to this framework are persistent health-compromising behaviours (PHCB). These behaviours arise through complex interactions between biological, psychological, social, and environmental influences. Because many of these behaviours initially provide short-term comfort or relief, they can gradually stabilise through reinforcing feedback mechanisms. Over time these feedback processes may evolve into what we describe as comfort loop syndrome (CLS), in which behaviours that initially reduce discomfort simultaneously generate biological, psychological, and social changes that increase the likelihood of repeating the same behaviours.
Understanding obesity through this behavioural organ systems perspective has several implications. First, it helps explain why behavioural patterns that contribute to obesity are often highly resistant to change. Behaviour is not simply the result of isolated individual choices, but the output of a relational behavioural organ system that integrates internal states and environmental influences. Once behavioural feedback loops have stabilised, change requires disruption of the reinforcing mechanisms that sustain them.
Second, this framework highlights the central role of the modern environment in shaping behavioural dynamics. Contemporary environments provide unprecedented access to highly rewarding foods, digital stimulation, and sedentary lifestyles. At the same time, behavioural norms spread through social networks, further reinforcing shared behavioural patterns. These environmental conditions increasingly bias behavioural organ systems toward persistent health-compromising behaviours.
Third, the framework illustrates how biological consequences of behaviour, including obesity itself, may become part of reinforcing feedback systems. Physiological adaptations, psychosocial consequences, and environmental responses can all strengthen the behavioural loops that contributed to the condition in the first place.
Importantly, this perspective does not deny the biological mechanisms involved in obesity. Rather, it integrates biological, behavioural, and environmental processes within a single conceptual framework. In this framework, biological processes both influence behaviour and are influenced by behaviour through dynamic feedback loops.
Taken together, this perspective suggests that effective prevention and treatment should focus not only on body weight or adipose tissue, but on the behavioural organ systems that generate persistent health-compromising behaviours. Interventions that disrupt comfort loop dynamics and strengthen healthier behavioural regulation may therefore play a central role in addressing obesity and other lifestyle-related health and social problems.
Ultimately, obesity may be better understood not simply as a disease of adipose tissue, but as a biological footprint of persistent behavioural dynamics unfolding within the behavioural organ systems of individuals living in modern environments.
References
- Van de Graaf RC, Van de Graaf PF. The Behavioural Organ. A relational executive system for the design and execution of human behaviour. J Health Behav Med Hist 2026-5.
- Van de Graaf RC. Comfort Loop Syndrome: a new framework for understanding and addressing the pandemic of lifestyle-related health societal problems. J Health Behav Med Hist 2025-22.
Reacties
5 reacties op “Reframing obesity: From adipose tissue disease to behavioural system outcome”
[…] de Graaf RC, Van de Graaf PF. Reframing obesity: from adipose tissue disease to behavioural system outcome. J Health Behav Med Hist […]
[…] final question raised in debates about the theory from the article Reframing obesity: from adipose tissue disease to behavioural system outcome [1] concerns the level at which the concept of disease should be […]
[…] de Graaf RC, Van de Graaf PF. Reframing obesity: from adipose tissue disease to behavioural system outcome. J Health Behav Med Hist […]
[…] de Graaf RC, Van de Graaf PF. Reframing obesity: from adipose tissue disease to behavioural system outcome. J Health Behav Med Hist […]
[…] de Graaf RC, Van de Graaf PF. Reframing obesity: from adipose tissue disease to behavioural system outcome. J Health Behav Med Hist […]